
Tekst voor Martijn
Home › Forums › Previous Months › 25 – February 2019: Life and Death › Tekst voor Martijn
- This topic has 2 replies, 3 voices, and was last updated 7 years, 3 months ago by
 DavidN.
DavidN.
-

kdrnicParticipantMarch 18, 2019 at 7:36 pm #2338So Tijn asked for my comment so I am giving it below. It is mostly on the realism of the first part of the game concerning appendicitis.
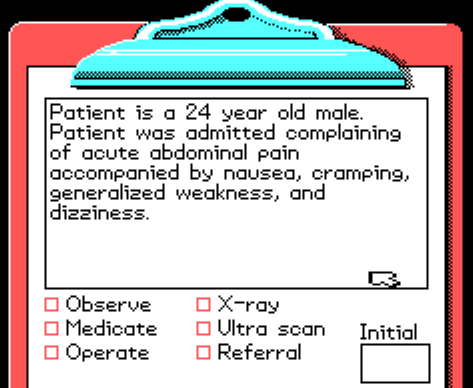
This history here is a bit lacking.
There is a standardised format we use. It starts with identification, then goes through chief complaint, history of present illness, past medical history, family history, social profile (includes alcohol use, occupational and environmental expositions), then concludes with the physical examination, the diagnostic hypotheses and the plan. During subsequent days in the hospital, or following office consults, smaller SOAP notes are written instead, those are Subjective (complaints and symptoms), Objective (physical and tests), Assessment and Plan.
In relation to the patient with acute abdomen, the most important bits will be age, sex, history of previous surgeries and a well collected history of present illness. The classical presentation for appendicitis is that of abdominal pain that starts diffuse, then through a couple days becomes more intense, and localised to the lower right quadrant. Together there is also usually fever and inappetence.
A history that does not match these characteristics makes one think of alternative diagnoses. The game seems particularly concerned with urinary tract calculi, but those usually present with a pain that already started very sharp, intense and localised, and usually more posterior and superior in relation to the expected position of the appendix in the lower right quadrant.
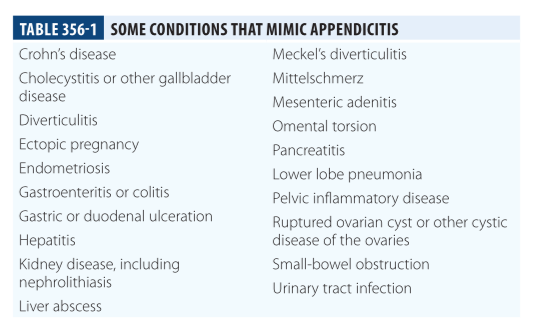
One extremely important alternative diagnosis is that of ectopic pregnancy, since it mimics the presentation very well, in both quality and localisation of the pain. In any woman of reproductive age it is necessary to consider and discard through a pregnancy test.Below are differentials for appendicitis in adults.
The game is correct to include the physical examination as an important step, though when well done it is more detailed – usually starts with auscultation for sounds of peristalsis, palpation is done first superficially then deep, and it goes first through the less painful regions. If appendicitis is suspected, then the physician must check for rebound tenderness in the lower right quadrant, called “Blumberg’s sign”, which is a sharp pain upon decompression of the abdominal wall.
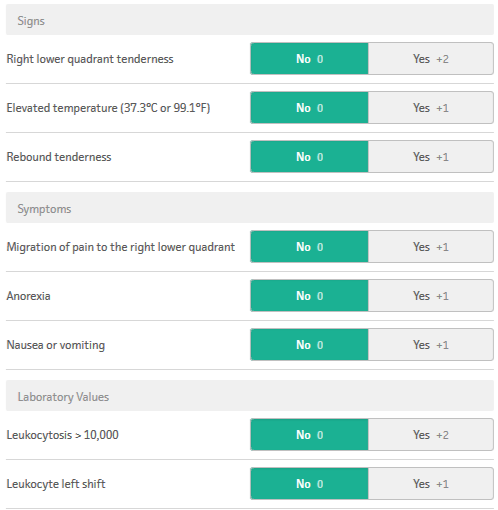
The game doesn’t include an option for lab tests, even though the presence of an abnormally high number of white cells in blood is highly characteristic of appendicitis and important in the approach to acute abdomen.Below is the Alvarado score, a clinical tool to predicit likelihood of appendicitis given clinical findings.
The game is from the 80s, so clearly its approach to radiology is quite outdated. I don’t know how correct it was back then, but nowadays the single best exam in the setting of acute abdomen is the ultrasound. It is safe since it doesn’t employ radiation (a concern since pregnancy is a differential) and it is the one which most often detects an enlarged appendix. The plain radiograph can only detect the presence of air in the cavity, and only if the appendix has ruptured, which is too late. In the case of calculi in the urinary tract, ultrasound won’t always find the stone, specially when they are behind bowels full of gas, but it tells whether the kidneys are dilated due to obstruction which defines urgency of intervention. The plain radiograph also misses calculi depending on the chemical composition. Computerised tomography is very useful when the diagnosis is unclear, and it can detect conditions like mesenteric ischaemia or diverticulitis quickly, and it rarely misses calculi of dangerous size. So nowadays for the acute abdomen the plain radiograph is of little use, the ultrasound is first choice and the CT next in line or first for selected cases. Of course the availability and image quality of CT has improved much since 1988 when this game was published.
This was all focused on diagnosis, but going next into the OR section of the game.
One thing which is a detraction from reality is that you perform both the task of the surgeon and of the anaesthesiologist. The latter is solely responsible for starting and stopping the anaesthetic, monitoring vital signs and taking actions to correct them when necessary. The real challenge of the anaesthesiologist is in fact not just employing anaesthesia, but keeping the patient alive through it. This leaves the surgeon to focus on his own task. It is also much more involved than merely turning the gas on. Due to the risk of aspiration of fluids and/or collapse of airways due to excessive relaxation, as well as the necessity to use oxygen and volatile anaesthetic agents in precise amounts, general anaesthesia occurs together with intubation of the patient. This requires the particular mechanical skill in inserting the tube, since it needs to be done quickly without causing too large a drop in oxygen saturation.
In select patients nowadays general anaesthesia is done without volatile agents, called Total IntraVenous Anaesthesia or TIVA. In rare cases also appendectomy has been performed with local anaesthesia, but the lower relaxation of the abdominal wall is a challenge.
In the game, the patient frequently needs administration of atropine or lidocaine, which is not usual in surgery of young individuals without co-morbidities.The operation itself is realistic and follows the correct order. There exist some variations to the procedure. The incision in the game is the McBurney, but occasionally the Lanz is used when the location of the appendix is very certain and the patient is lean. When going through the subcutaneous most often surgeons will choose to cut with electrocautery tool rather than the scalpel, but this is a matter of personal preference. When the colon is closed in the game the purse-string suture is performed but simpler methods are also safe when the appendix is not too inflamed.
Lastly, many appendectomies today are performed laparoscopically, a procedure in which small incisions are made, one of which is used to inject air, another for a fibre optics combination of camera and light and a number of others to insert long, thin tools, allowing less invasive procedures. Depending on the location of the appendix and the thickness of the abdominal wall the aesthetic result is better and the patient may recover more quickly.
The second surgery in the game is the aortic aneurysm repair. It is still an intimidating procedure, carrying a 3% mortality in the fittest patients, although preventing the much higher mortality from ruptured aneurysm. The open procedure remains similar nowadays, but there is also the possibility of endovascular repair. In this variation, instead of open surgery a catheter is introduced through a peripheral artery and guided to the aorta with the help of real time fluoroscopy, once in situ a device is triggered which opens and installs the prosthesis which is not dissimilar to the more familiar coronary stent, although its function is to keep the wall from rupturing rather than collapsing as in the case of the latter. This technique unfortunately is also risky, so it is still a challenging condition.
I believe this is a good summary of the realism and accuracy of the game, open to further questions.
March 19, 2019 at 2:42 pm #2342Thanks, this is very interesting information!
You must be logged in to reply to this topic.
Home › Forums › Previous Months › 25 – February 2019: Life and Death › Tekst voor Martijn
